At St. George's we use two types of automatically marked question. We use multiple choice questions of the stem and 5 branch type, where each stem may be True or False, usually referred to as "MCQs". We use extended matching items questions, where there is a scenario and any number of questions with answers chosen from a long list, usually referred to as "EMIs". In our usual practice, MCQs have negative marking, i.e. you get +1 for a right answer and -1 for a wrong answer, and EMIs do not have negative marking.
Each branch is True or False.
1. In an experiment to compare two treatments, advantages of random
allocation include:
(a) the sample may be referred to a known population.
(b) the experimenter will not know what treatment the subject will receive
before recruiting them into the study.
(c) the likely size of errors can be estimated.
(d) the two groups will be similar, apart from treatment.
(e) treatments are assigned according to the characteristics of the subjects.
2. The following are qualitative variables:
(a) sex.
(b) parity (number of previous pregnancies).
(c) diastolic blood pressure.
(d) diagnosis.
(e) height.
3. The following are continuous variables:
(a) arm circumference.
(b) age last birthday.
(c) exact age.
(d) peak expiratory flow rate.
(e) family size.
4. When a distribution is skew to the right:
(a) the median is greater than the mean.
(b) the distribution is always unimodal.
(c) the tail on the left is shorter than the tail on the right.
(d) the standard deviation is always less than the variance.
(e) the majority of observations are less than the mean.
5. In a randomised double-blind trial to compare a new analgesic with
placebo for the control of pain in arthritis, subjects reported less pain while
using the analgesic and the difference in pain scores between the two regimes
was highly significant (P=0.002). We can conclude that:
(a) an important clinical advance has been made.
(b) there is good evidence that the drug reduces pain.
(c) the drug is a very effective analgesic.
(d) it is unlikely that the results would have been obtained if the drug were
totally ineffective.
(e) The difference between mean pain scores on the two regimes was 0.002.
6. In a randomised double-blind trial to compare a new analgesic with
ibuprofen, a standard treatment, for the control of pain in arthritis, the
difference in pain scores between the two regimes was not significant. We can
conclude that:
(a) the new drug is useless.
(b) there is no difference in analgesia between the two drugs.
(c) the trial has failed to demonstrate a difference in analgesia.
(d) the difference between the drugs is very small.
(e) there are no important differences in the analgesic properties of the
drugs.
7. A study was carried out to compare chemotherapy given at home with
outpatient treatment for colorectal cancer patients. 42 patients were treated
at outpatient clinic and 45 at home. Treatment related toxicity was similar in
the two groups (difference 7% (95% confidence interval -12% to 26%)), but there
were more voluntary withdrawals from treatment in the outpatient group than in
the home group (14% v 2%, difference 12% (1% to 24%)). Satisfaction with the
communication with the nurse and the doctor were scored on scales from 1 to
100, with higher scores representing greater satisfaction. For communication
with the nurse, outpatients' scores had mean (SD) equal to 82 (25) and for home
patients these were 100 (0), difference in means (95% CI) -18 (-26 to -9). For
communication with the doctor, the corresponding statistics were 70 (26), 70
(22), and 1 (-12 to 14) (The difference is 1 rather than 0 is because of
rounding errors.) (BMJ 2001;322:826)
(a) The trial is double blind.
(b) Patients should give written consent before the trial began.
(c) There is little or no evidence that voluntary withdrawal differs between
home and outpatient treated colorectal cancer patients.
(d) All the home treated patients rated their satisfaction with communication
with the nurse as 100.
(e) We can conclude that, in the population of colorectal cancer patients,
there is no difference in satisfaction with communication with the doctor for
between home and outpatient treated patients.
8. In the trial of home treatment for colorectal cancer (Question 7), the
difference in treatment related toxicity was 7% (95% confidence interval -12%
to 26%).
(a) If we took another sample, there is a 95% probability that the difference
in risk obtained from that sample would lie between -12 and 26.
(b) We estimate that the difference in treatment related toxicity in the
population of patients from which this sample is drawn is between -12 and
26.
(c) The population difference would be zero if the two treatments had the same
effect.
(d) The probability that the relative risk in the sample lies between -12 and
26 is 95%.
(e) The treatments would not be significantly different at the 5% level.
For each question choose one answer from the following list:
At least 28 randomised, controlled trials have compared outcomes of surgery for rectal cancer combined with preoperative or postoperative radiotherapy with those of surgery alone. The results of these trials were combined to give a more balanced view of the total evidence and to increase statistical precision. Overall survival was only marginally better in patients who were allocated to radiotherapy than in those allocated to surgery alone (62% vs 63% died; p=0.06). Rates of apparently curative resection were not improved by preoperative radiotherapy (85% radiotherapy vs 86% control). Yearly risk of local recurrence was 46% (SE 6) lower in those who had preoperative radiotherapy than in those who had surgery alone (p=0.00001), and 37% (10) lower in those who had postoperative treatment than those who had surgery alone (p=0.002). Fewer patients who had preoperative radiotherapy died from rectal cancer than did those who had surgery alone (45% vs 50%, respectively, p=0.0003), but early (1 year after treatment) deaths from other causes increased (8% vs 4% died, p<0.0001). (Lancet 2001; 358: 1291-304)
9. What is represented by "SE"?
10. How strong is the evidence that radiotherapy increases survival?
11. How strong is the evidence that preoperative radiotherapy reduces recurrence?
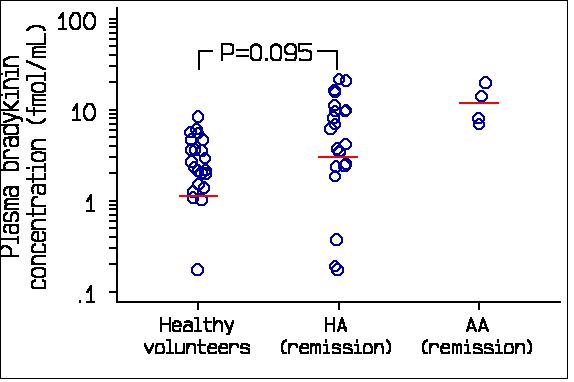
Bradykinin is believed to be the main mediator of symptoms in hereditary (HA) and acquired (AA) angiooedema. Plasma bradykinin concentrations were measured in 22 patients with HA and in 22 healthy volunteers of similar age and sex distribution. Four patients with AA were also studied. (Lancet 1998; 351: 1693-97.) A figure similar to the following was included:
12 What term describes the vertical scale?
13. Which term best describes the evidence that HA patients have raised plasma bradykinin?
To determine whether a noradrenergic mechanism contributes to the anorexigenic effect of GLP-1 on the neonatal chick, food intake was measured after central administration of norepinephrine (NE). (Pharmacology, Biochemistry and Behavior 2001; 70: 251-255.) A figure similar to the following was produced:
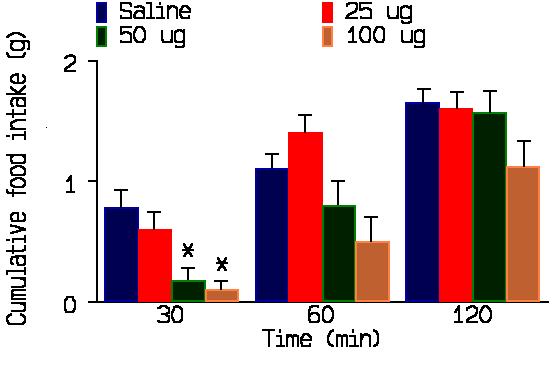
Fig. 1. Cumulative food intake over a 2-h period after ICV injection of norepinephrine or saline in 2-day-old chicks. Values are means +/-S.E.M. *P<.05 compared to control saline. Numbers of birds used were: 10 (saline), 9 (25 g), 8 (50 g) and 8 (100 g).
14. What kind of graph is this?
15. What do the thin vertical lines represent?
16 How strong is the evidence that a dose of 25 micrograms reduces food intake compared to saline?
To assess the overall efficacy of voice therapy for dysphonia (hoarseness) 204 outpatients were allocated to six weeks of either voice therapy or no treatment. Treatment could be indirect, for example, involving discussion of issues of vocal hygiene or of lifestyle impinging on voice production. Equally, patients could be invited to practise techniques related to their vocal symptoms for example, improving breath support for vocal production or altering vocal onset in favour of "softer" vocal attack. The outcome measures included ratings of laryngeal features, Buffalo voice profile, amplitude and pitch perturbation. These were assessed from a digital tape recording of the patient's reading of a standard passage by a speech and language therapist who did not know the patient's treatment group. At the final visit, the mean (SD) for pitch perturbation was 3.1 (2.4) for the treated and 2.4 (1.4) for the untreated patients, P = 0.212. (Scores are all positive, high score means a poor voice.) (BMJ 2001; 323: 658-661)
17. What method of allocation to treatment should be used in such a study?
18. Which term best describes the degree of blindness in the study?
19. What shape of distribution do the data suggest for the pitch perturbation?
20. How strong is the evidence that voice therapy improves pitch perturbation in dysphonic patients?
Back to Research and Critical Skills Course Page.
This page maintained by Martin Bland.
Last updated 29 June, 2004.