 D
D
Stenosis or narrowing of the carotid artery in the neck greatly increases the risk of stroke by blocking the flow of blood to the brain. The standard treatment is to graft a piece of vein in place of the blocked section of artery, endarterectomy. Most of the patients are frail and elderly. This is an invasive procedure carried out under general anaesthesia and it might be preferable if this can be avoided. Several trials have been done of angioplasty, where a wire is inserted into the artery and use to guide an inflatable balloon to the site of the stenosis. There it can be inflated to widen the narrowed artery. To keep the artery open, a stent is often left in place. This is a wire mesh tube which sits in the artery.
There are short-term risks to both procedures and there may be peri-operative deaths related to anaesthesia problems and there may be strokes because a piece of plaque is dislodged from the artery and blocks a blood vessel leading to the brain.
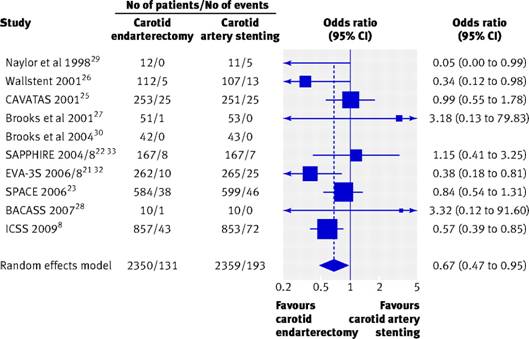
Meier and colleagues (2010) reported a meta-analysis of randomised trials comparing endarterectomy versus stenting for carotid artery stenosis to prevent death or stroke.
They identified ten trials which provided data on the short-term outcome of death or stroke, and one of their meta-analyses is shown in the following figure, taken from the BMJ:
(CAVATAS and ICSS are my own trials — Martin.)
In this exercise we shall use CMA2 to carry out this meta-analysis.
Start CMA2.
Questions
Question 1: How should we put in the data from the BMJ graph?
Question 2: On the CMA2 data entry screen, what is missing for the study of Brooks et al. (2004)? Why is it missing?
Run analyses.
Question 3: On the CMA2 analysis screen, what is missing for the study of Brooks et al. (2004)? Why is it missing?
Question 4: How can we save this output onto a file for future use?
Question 5: Is the default fixed effects model the right one to use?
Draw the high resolution forest plot.
Question 6: How could we improve the forest plot?
Question 7: How could we improve the forest plot further?
Question 8: How could we label the combined estimate as "Fixed" on the forest plot?
Question 10: How can we save the forest plot image for future use in a word processing file?
Question 11: How could we check for any evidence of publication bias?
In the CAVATAS/ICSS team, the hypothesis was put forward that, in the time between these two studies, surgical techniques had improved. This had increased the difference between endarterectomy and stenting in the 30 day follow-up.
Question 12: What method could we use to examine the effect of calendar time on treatment effect?
Question 13: How can we do this in CMA2?
Meier P, Knapp G, Tamhane U, Chaturvedi S, Gurm HS. Short term and intermediate term comparison of endarterectomy versus stenting for carotid artery stenosis: systematic review and meta-analysis of randomised controlled clinical trials BMJ 2008; 340: c467.
To Martin Bland's M.Sc. index.
This page maintained by Martin Bland.
Last updated: 19 February, 2010.